Each year, an estimated 400,000 children and adolescents aged between 0 and 19 years develop cancer, the most common types being leukemia, brain cancer, lymphoma and solid tumours such as neuroblastomas. Owing to rapid advances in medical treatment, and supportive care, around 80% of these children will survive well into their adult years; a huge increase since the mid-1970’s. However, beyond the statistics lies the physical and psychosocial challenges that come with cancer survivorship. Survivors face the very real threat of recurrence and the risk of developing a second cancer.
Childhood cancer survivors are at increased risk of developing a recurrence of their primary cancer compared with the general population’s risk of developing cancer. In addition to this, childhood survivors are 5 times more likely to develop a second cancer, with elevated risk continuing into the sixth decade of life.
For survivors and their families who have already braved the physical and emotional battle against cancer, the threat of cancer recurrence and risk of developing a second cancer can manifest psychological distress, including anxiety and fear of death as well as depressive symptoms such as the loss of hope for recovery and difficulties dealing with their disability. Survivors may also experience appetitive difficulties such as anorexia, poor body image and anxiety dealing with their pain.
Our recent study entitled; “It just never ends”: Childhood cancer survivors’ perceived psychosocial impacts of recurrence and second cancer” examines childhood cancer survivors and their families’ perspectives on being diagnosed with a second cancer, or a recurrence of their primary cancer.
Strong emotional and psychological impacts
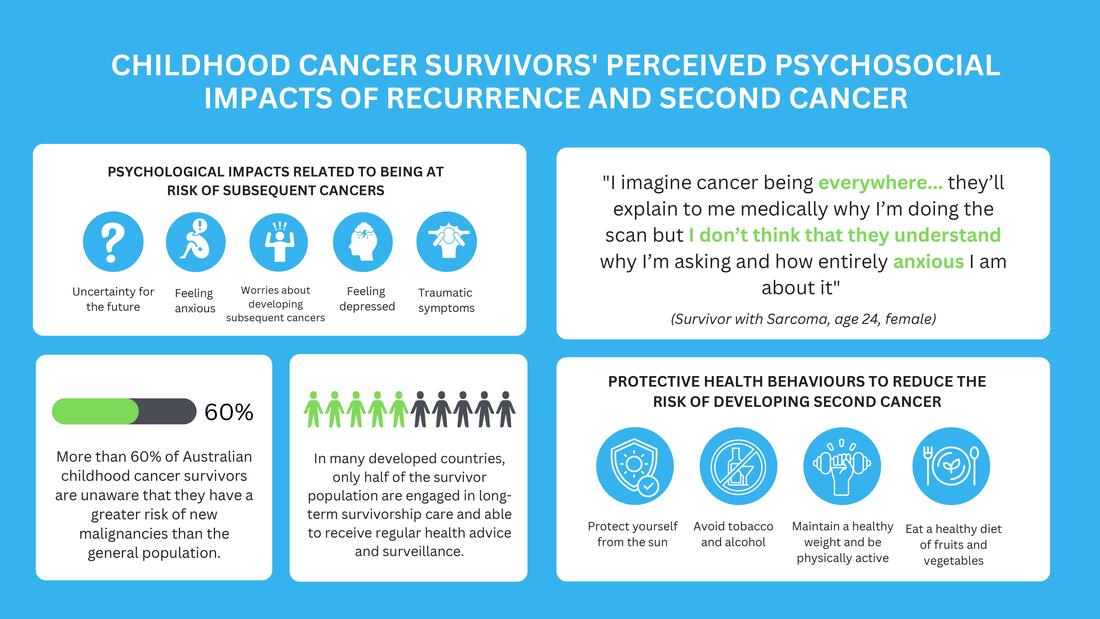
Most participants experienced feelings of helplessness, anxiety, worry and trauma when their cancer recurred; a 26-year-old, female survivor with secondary carcinoma voiced “There has been a lot of depression…and chronic pain”. Other patients described their experience to be like a “kind of rollercoaster” and felt as though they were entering a figurative “no man’s land”. More so, some survivors reported experiencing severe post-traumatic stress disorder (PTSD), with others developing strong phobias for hospitals and needles. The study further highlights how survivors felt that a great deal of their pressure and anxiety stemmed from having to make important medical decisions without being given enough time to fully process the risks and side effects of the cancer treatment.
Considering the psychosocial impact of cancer, it is understandable why some patients may see avoidance as a way of ‘moving on’ from their cancer experience or regaining a sense of normalcy. Nonetheless, literature shows that poor awareness of late effects is linked to low-risk perceptions, poor adoption of health behaviours and in turn, an increased risk of recurrence or second cancer.
Health behaviour adherence
Interestingly, the study reported that despite having experienced a primary cancer, as well as a recurrence or second cancer, some survivors still felt ambivalent or even reticent towards receiving information about the cancer-related health risks that they may develop. Some survivors also resisted adopting protective health behaviours, such as avoiding alcohol, smoking, and using sun protection. In fact, the use of sun protection is the least practiced health precaution among childhood cancer survivors despite evidence that the majority of second cancers are skin neoplasms.
Childhood cancer survivors are at increased risk of developing a recurrence of their primary cancer compared with the general population’s risk of developing cancer. In addition to this, childhood survivors are 5 times more likely to develop a second cancer, with elevated risk continuing into the sixth decade of life.
For survivors and their families who have already braved the physical and emotional battle against cancer, the threat of cancer recurrence and risk of developing a second cancer can manifest psychological distress, including anxiety and fear of death as well as depressive symptoms such as the loss of hope for recovery and difficulties dealing with their disability. Survivors may also experience appetitive difficulties such as anorexia, poor body image and anxiety dealing with their pain.
Our recent study entitled; “It just never ends”: Childhood cancer survivors’ perceived psychosocial impacts of recurrence and second cancer” examines childhood cancer survivors and their families’ perspectives on being diagnosed with a second cancer, or a recurrence of their primary cancer.
Strong emotional and psychological impacts
Most participants experienced feelings of helplessness, anxiety, worry and trauma when their cancer recurred; a 26-year-old, female survivor with secondary carcinoma voiced “There has been a lot of depression…and chronic pain”. Other patients described their experience to be like a “kind of rollercoaster” and felt as though they were entering a figurative “no man’s land”. More so, some survivors reported experiencing severe post-traumatic stress disorder (PTSD), with others developing strong phobias for hospitals and needles. The study further highlights how survivors felt that a great deal of their pressure and anxiety stemmed from having to make important medical decisions without being given enough time to fully process the risks and side effects of the cancer treatment.
Considering the psychosocial impact of cancer, it is understandable why some patients may see avoidance as a way of ‘moving on’ from their cancer experience or regaining a sense of normalcy. Nonetheless, literature shows that poor awareness of late effects is linked to low-risk perceptions, poor adoption of health behaviours and in turn, an increased risk of recurrence or second cancer.
Health behaviour adherence
Interestingly, the study reported that despite having experienced a primary cancer, as well as a recurrence or second cancer, some survivors still felt ambivalent or even reticent towards receiving information about the cancer-related health risks that they may develop. Some survivors also resisted adopting protective health behaviours, such as avoiding alcohol, smoking, and using sun protection. In fact, the use of sun protection is the least practiced health precaution among childhood cancer survivors despite evidence that the majority of second cancers are skin neoplasms.
What can survivors and health professionals do to help?
And so, the question remains, how do we mitigate these risks? The literature suggests that by incorporating health-education programs into survivorship care survivors may feel assured that solutions are available to prevent or intervene early and can contribute to a perception of ‘preparedness’ in the event of cancer recurrence, and/or the development of a second cancer. To ensure knowledge dissemination and optimal receptiveness, these programs should be delivered in a way that is educational and places emphasis on causal pathways that can be avoided or minimised and positive health management, rather than simply describing subsequent cancer risks.
With more and more children surviving childhood cancer, it is critical that recurrence and second cancer risk information is not only conveyed accurately, but also in a manner which will reduce fear of cancer recurrence and increase health behaviours for the prevention and early intervention of subsequent disease. Together we look forward to building a path towards a better health future for patients and their families.
You can read the full paper here.
Blog post written by Alexia Paglia and Dr Jordana McLoone.
And so, the question remains, how do we mitigate these risks? The literature suggests that by incorporating health-education programs into survivorship care survivors may feel assured that solutions are available to prevent or intervene early and can contribute to a perception of ‘preparedness’ in the event of cancer recurrence, and/or the development of a second cancer. To ensure knowledge dissemination and optimal receptiveness, these programs should be delivered in a way that is educational and places emphasis on causal pathways that can be avoided or minimised and positive health management, rather than simply describing subsequent cancer risks.
With more and more children surviving childhood cancer, it is critical that recurrence and second cancer risk information is not only conveyed accurately, but also in a manner which will reduce fear of cancer recurrence and increase health behaviours for the prevention and early intervention of subsequent disease. Together we look forward to building a path towards a better health future for patients and their families.
You can read the full paper here.
Blog post written by Alexia Paglia and Dr Jordana McLoone.
 RSS Feed
RSS Feed